Greek physicians were prescribing sunshine for melancholy and weak limbs long before anyone understood why it might help. They had the instinct right and the mechanism completely wrong. The real breakthrough wasn’t discovering that light heals; it was learning to control it down to a single wavelength and a measured dose.
That control is what separates a tanning bed from a treatment. A modern clinician can isolate one colour, point it at a square centimetre of skin or a tumour buried in the throat, and leave everything around it untouched. The equipment has come down in size and price too, which is how something once bolted to a hospital wall now sits quietly on bedside tables.
Skin first, and the youngest patients
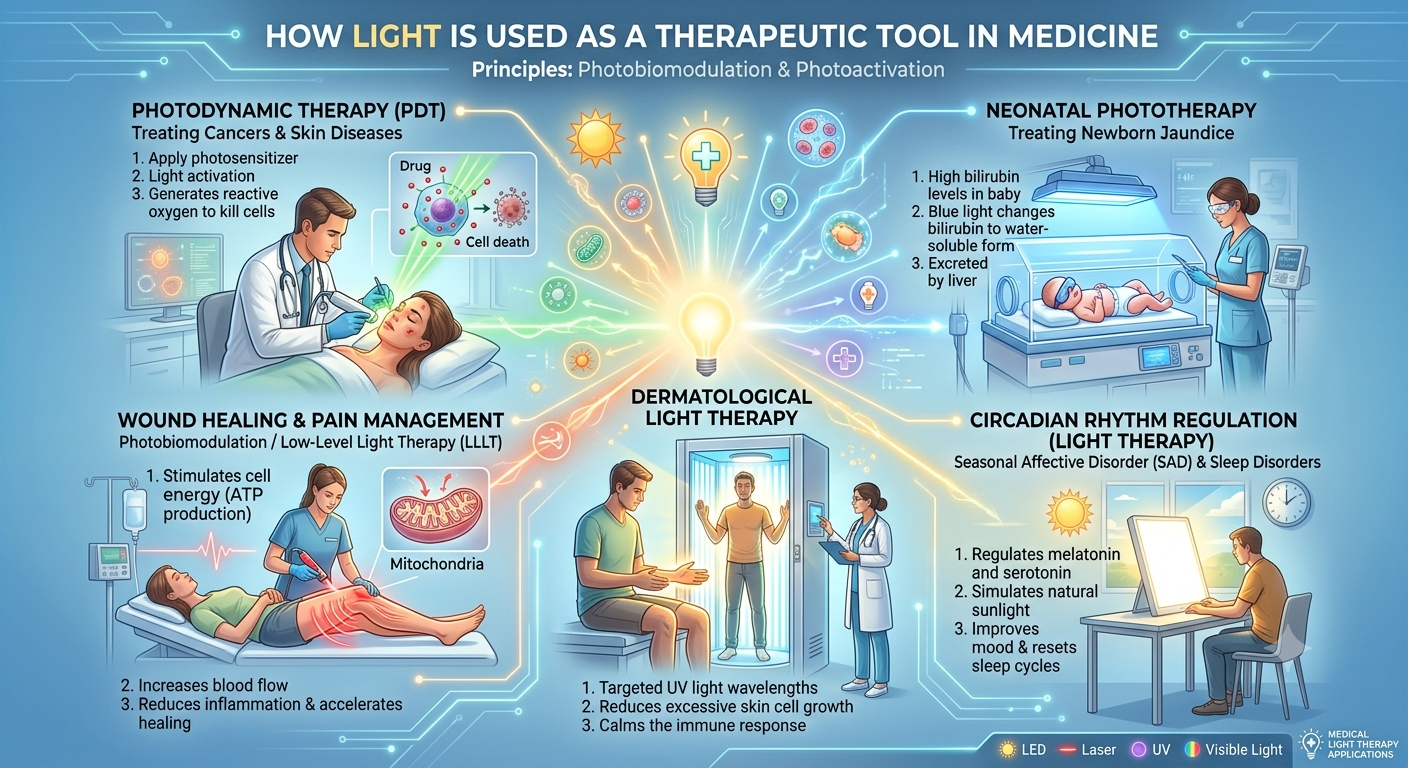
Dermatology got here first and never really left. The workhorse is narrowband ultraviolet B at around 311 nanometres, which slows the runaway skin-cell turnover behind psoriasis and settles the inflammation of eczema and vitiligo. Patients stand in a tube-lined booth for a few minutes at a time, the dose nudged up gradually over weeks so the skin adapts instead of burning.
Newborns get the gentle end of the spectrum. The blue glow over a jaundiced baby, often delivered through a fibre-optic “bili blanket” wrapped against the skin, breaks down the bilirubin that turns them yellow. Anyone who reads up on what is phototherapy tends to come away surprised at how many separate jobs hide behind one calm-sounding word, each tied to its own colour and target.
When the target is the brain
Light doesn’t stop at the skin. Routed through the eyes, it resets the body clock that governs sleep and mood, which is the whole premise behind the bright boxes sold for seasonal affective disorder. The standard routine is twenty minutes to half an hour beside a 10,000-lux lamp, taken early in the morning before the day properly gets going, when the body clock is most open to a nudge.
The NHS is admirably unsentimental about the evidence, calling it thin and steering people toward a GP rather than a checkout. Users tend to be more enthusiastic than the trials are. It’s cheap to try and hard to overdo, which probably explains why the lamps keep selling either way.
The same clock-shifting logic reaches well past the winter blues. Night-shift workers and jet-lagged travellers use timed light to drag themselves onto a new schedule, and sleep clinics combine it with planned darkness to push a stubborn rhythm earlier or later.
Light as a scalpel
The most striking use turns light into something close to a guided weapon. In photodynamic therapy a patient is given a photosensitising drug, Photofrin or 5-ALA among them, that collects in cancer cells before a red light near 630 nanometres is shone onto the spot. The drug soaks up that light and releases a short, violent burst of reactive oxygen that kills the cell from the inside, while the tissue around it is largely left alone.
Cancer Research UK makes the neat part plain: the drug and the light are nearly inert on their own, and the damage only lands where the two overlap. So tissue a few millimetres away usually comes through fine. That selectivity is why it works on skin, mouth and oesophageal cancers, with fibre-optic cables threaded down endoscopes to reach the deep ones.
Colour is the lever behind all of it. Blue and ultraviolet stay shallow while red and near-infrared travel further into tissue, and a broad overview of light therapy lays out which conditions actually respond. None of this is risk-free, mind: UV adds up toward skin cancer, the bright boxes can tip bipolar patients into mania, and plenty of common medicines leave skin touchy under light.
The newest devices are mostly about smarter dosing. Sensors now read how skin or tissue responds and adjust the output in real time, and wearable LED patches are already pulling parts of the treatment out of the clinic and into the spare room. A handful of systems now log every session automatically, so a patient’s dose history follows them from one appointment to the next.
Folk advice about catching some sun became one of the more precise tools a doctor owns, and it did it without much fanfare. Cheaper LEDs, better sensors and sharper aim will keep widening what a handful of well-placed photons can quietly fix.

